
骨关节炎(专业级)
骨关节炎(OA)是一种很常见的退行性关节病,其特征在于关节软骨的逐渐磨损、增生和功能障碍。
英文名称:Arthritis,Osteoarthritis,Degenerative Joint Disease
定义
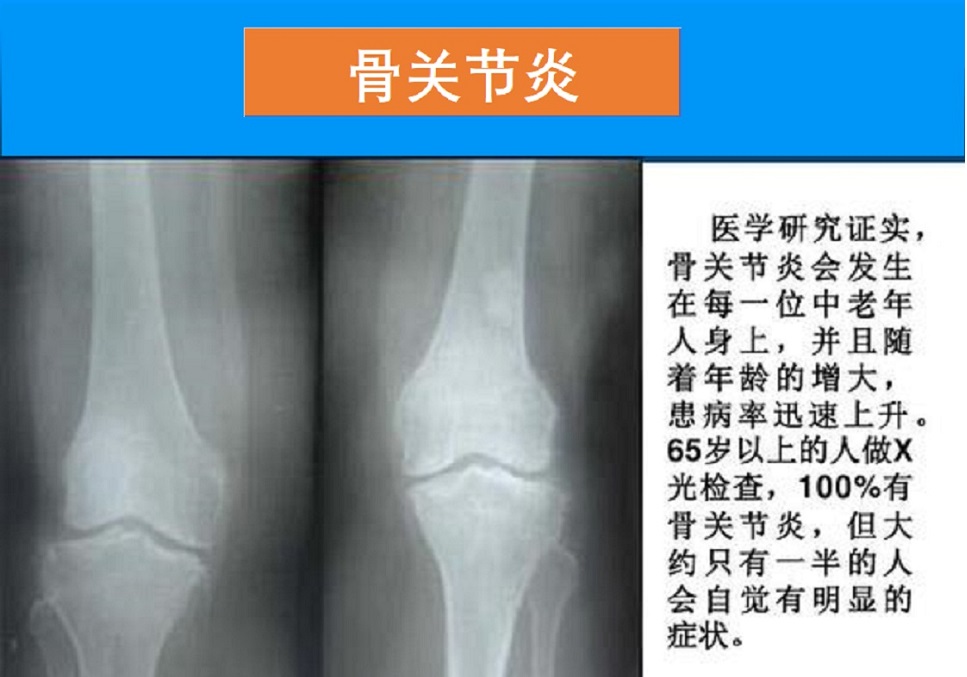
骨关节炎(OA)是一种很常见的退行性关节病,其特征在于关节软骨的逐渐磨损、增生和功能障碍。本病多见于中老年人群,好发于负重关节及使用量较多的关节(颈椎、腰椎、膝关节、髋关节等),引起关节疼痛、僵硬、肿胀和畸形等,也是导致残疾的主要原因之一。病因
关节磨损是人体老化的一部分。软骨是覆盖关节区域的光滑组织,它为骨头提供了缓冲,支持关节顺利地工作。随着时间的推移,关节受到的应力、压力和冲击会拖垮软骨,损伤不断恶化。最终,软骨可能完全磨损,留下骨头摩擦在一起而产生疼痛等症状。此外,关节损伤、肌肉无力,或其他疾病可能使病情加重。骨关节炎发病机制与老化、代谢密切相关,包括氧化应激,炎症和线粒体障碍等。
风险因素
OA在绝经后女性,以及老年人中较易发生。其他可能增加OA机会的因素包括:
- 超重或肥胖
- 家族病史
- 某些内分泌、代谢、或神经性疾病
- 职业运动员或体育活动,增加了关节应力
- 缺血性坏死,缺乏血流引起
- 涉及关节的创伤或手术,尤其是软骨
症状
在支撑重量的较大关节如脊柱、髋关节和膝盖中,骨关节炎是最常见的。在手和脚等活动性关节中也很常见。常见症状包括:
- 轻度至重度的关节疼痛,特别是过度使用或长时间休息之后
- 关节吱吱声
- 肿胀、僵硬,影响关节活动,尤其在早上
- 运动后,僵硬降低
并发症
骨关节炎是随着时间推移恶化的退行性疾病。关节疼痛和僵硬可能严重影响日常生活,许多活动变得困难。疗法
骨关节炎不能治愈。治疗的重点是减轻症状和缓解软骨损伤。当软骨磨损时,骨摩擦会导致疼痛和炎症。
综合选项可包括如下:
调整饮食和生活方式
- 健康饮食,如地中海饮食法
- 保持健康体重
- 坚持适当的运动锻炼
营养与草本综合干预
以下是基于循证医学和循证营养学有关文献综合的结果。
有助于防控骨关节炎的营养和草本补充剂,主要包括如下:
Nutrients译文:
1.氨基葡萄糖:
氨基葡萄糖(简称氨糖)是构成糖胺聚糖和蛋白聚糖的化合物的成分,它们有助于将水截留在软骨基质中,为软骨提供所需的灵活性和弹性1。在实验室模型中,氨糖已被证明具有抗炎作用。研究表明,剂量高达1500 mg时,它可以降低骨关节炎(OA)症状的严重程度2,3。此外,临床前研究表明,氨糖可以通过调节软骨细胞合成软骨结构成分来支持软骨完整性4。氨糖在维持关节润滑方面也起着至关重要的作用1。.
2.硫酸软骨素:
这是一种存在于骨骼、软骨、肌腱、韧带和皮肤中的复杂糖分子5。硫酸软骨素(简称软骨素)有助于软骨保持水分,增加润滑和弹性。一项研究发现,关节炎关节的软骨样品的硫酸软骨素浓度低于健康关节的样品6。在实验室研究中,硫酸软骨素减少炎症,促进骨和软骨的分解和新形成之间的健康平衡5。软骨产生细胞的实验室研究表明,氨糖和硫酸软骨素可能以互补的方式保护软骨7。
在一项针对350名膝关节骨性关节炎患者的双盲随机研究中,每天1200 mg硫酸软骨素可减轻疼痛8。在另一项针对162名手关节骨性关节痛患者的随机、安慰剂对照、双盲研究中,软骨素与安慰剂相比可减轻疼痛并改善功能9。一项涉及600多名膝关节骨性关节炎患者的对照试验用200mg塞来昔布或400mg软骨素加500mg氨糖治疗参与者,每天三次,为期六个月。氨糖和软骨素组的疼痛、僵硬和关节肿胀改善情况与塞来昔布组相似10。
一项随机对照试验比较了138名膝关节骨性关节炎患者每天1200mg软骨素和每天200mg塞来昔布的疗效。经过两年的治疗,两个治疗组的肿胀和症状(如膝盖疼痛和僵硬)得到了类似的缓解。然而,MRI测量显示,服用软骨素的患者软骨体积损失显著减少11,12。在一项随机临床试验中,605名患有膝关节骨性关节炎的参与者,每天接受800mg软骨素和1500mg硫酸氨糖联合治疗的组,两年后关节间隙变窄的情况比单独接受安慰剂或任一补充剂的组要少13。
3. 透明质酸:
透明质酸是软骨的组成部分,主要存在于皮肤中14。高度纯化的透明质酸用于关节内注射,暂时缓解关节炎症状。口服透明质酸后,OA患者的关节疼痛减轻且功能增强15。
在一项研究中,40名关节不适的健康受试者在90天内每天食用添加透明质酸或纯酸奶的酸奶。酸奶中含有透明质酸的受试者膝关节肌肉力量有所改善16。在另一项研究中,20名40岁或40岁以上的膝关节骨性关节炎受试者每天服用80mg提供60%透明质酸或安慰剂的鸡冠提取物,持续8周。服用透明质酸补充剂的参与者在某些疼痛和功能方面比服用安慰剂的参与者有更大的改善17。
4. 鳄梨大豆不皂化物:
鳄梨大豆不皂化物是一种由大豆油和鳄梨油制成的天然提取物,可以通过调节OA的多种途径来减少OA的进展18。鳄梨/大豆不皂化物还具有软骨保护作用,减轻疼痛和僵硬,改善关节功能,并可能减少对止痛药的依赖19。
在一项随机、双盲、安慰剂对照试验中,14名患有OA和关节痛的妇女,与安慰剂相比,鳄梨/大豆不皂化治疗四个月可减少疼痛,提高生活质量,并减少止痛药的使用20。在一项前瞻性、随机、双盲研究中,399名髋关节骨性关节炎患者接受了300mg/天鳄梨大豆不皂化物或安慰剂治疗。治疗组显示关节结构发生了改变,这表明鳄梨/大豆不皂化物可能在阻止髋关节OA进展方面发挥临床作用21。需要更多的临床研究佐证。
5.欧米伽3脂肪酸:
- 鱼油:EPA和DHA可减轻炎症,有助于缓解OA相关症状。256人体研究表明,补充鱼油可减轻一些OA症状,尽管总体证据相对较弱,需要进行质量更高的研究22,23。在动物研究中,ω-3脂肪酸降低了软骨降解的标志物。其他OA动物模型发现,补充ω-3脂肪酸可以改善日常活动能力和身体残疾症状24,25。
- 磷虾油:与鱼油一样,它是海洋动物ω-3脂肪酸的来源。然而,与鱼油不同的是,磷虾的ω-3脂肪酸存在于磷脂的天然基质中,与每个细胞膜中的磷脂相似。这种组成特性可能有助于从磷虾油中有效吸收ω-3脂肪酸32。此外,磷虾富含的虾青素,已证明具有抗炎、抗氧化和软骨保护作用33,34。对磷虾油与鱼油的吸收和生理作用进行的临床前和临床研究综述发现,磷虾油似乎比鱼油具有更高的生物利用度。磷虾油和鱼油的生化和代谢作用似乎也有所不同。然而,在就磷虾油和鱼油的不同影响得出确切结论之前,需要进行更多的独立研究33。
然而,并非所有磷虾油治疗OA的试验都显示出益处;一项研究发现,每天2g磷虾油与安慰剂相比没有任何益处37。
6.胶原蛋白II型:
胶原蛋白是哺乳动物中含量最高的蛋白质,是全身结缔组织(包括骨骼和软骨)的主要结构蛋白38。临床试验表明,补充胶原蛋白肽(通常来源于水解胶原蛋白)可以缓解OA症状。在一项随机对照试验中,研究了补充胶原蛋白肽是否有助于治疗膝关节骨性关节炎,参与者被给予补充胶原蛋白肽或安慰剂13周。服用胶原蛋白补充剂的人报告说,与服用安慰剂的人相比,其生活质量和疼痛都有所改善39。
未变性的II型胶原是一种天然形式的胶原,可以从鸡软骨中提取40。一些研究人员认为,摄入后,未变性的Ⅱ型胶原会与肠道中的免疫系统部分(即肠道相关淋巴组织)相互作用。通过这种相互作用,未变性的II型胶原可能有助于训练免疫细胞不攻击胶原肽,类似于受关节炎影响的关节中软骨分解时可能暴露的胶原肽41,42。不过,需要进行更多的研究来阐明补充II型胶原支持关节健康的机制。
一项涉及52名膝关节骨性关节炎患者的临床试验发现,与每天两次的750mg氨糖和600mg软骨素相比,每天两次服用5mg未变性的II型胶原,在治疗90天后,疼痛、身体功能和僵硬都得到了改善43。在另一项随机安慰剂对照试验中,39名膝关节骨性关节炎患者每天接受1500mg对乙酰氨基酚或1500mg对乙氨基酚加10mg未变性的II型胶原治疗,为期三个月。与单独使用对乙酰氨基酚组相比,使用对乙酰氨酚和胶原蛋白组在行走、功能和生活质量方面的关节疼痛改善更大44。
在另一项多中心、随机、双盲、安慰剂对照试验中,190名膝关节骨性关节炎受试者接受了40mg含有未变性II型胶原、1500mg氨糖和1200mg软骨素的制剂或安慰剂治疗180天。与其他组相比,服用胶原蛋白的组在疼痛、僵硬和功能方面表现出更大的改善45。
7. 甲磺酰甲烷(MSM):
作为含硫化合物,MSM可以减轻炎症和疼痛,并抑制与OA相关的变性。一项动物模型研究发现,MSM减少了软骨退化46。在一项前瞻性、随机、双盲、安慰剂对照试验中,49名膝关节骨性关节炎受试者服用1125mg MSM,每天三次,持续12周,改善了骨性关节炎的疼痛和身体功能47。在一项随机、双盲、安慰剂对照试验中,50名膝关节骨性关节炎疼痛患者接受3000mg MSM或安慰剂治疗,每天两次,持续12周。与安慰剂相比,补充MSM可减少疼痛和身体损伤48。
另一项随机、双盲、安慰剂对照研究涉及100名髋关节和/或膝关节OA患者,发现与安慰剂相比,连续26周每天服用6g MSM可减轻疼痛并改善功能表现49。在另一项试验中,37名膝关节OA患者每天三次服用两片含有500mg氨糖、400mg软骨素和250mg MSM的片剂。完成研究的患者报告疼痛和功能得到改善,关节活动度逐渐改善50。需要在更低剂量和更大样本量下进行进一步研究,以确定含硫化合物是否可用于治疗OA。
8. S-腺苷蛋氨酸(SAMe):
SAMe是一种体内天然存在的化合物,通过充当甲基供体有助于促进许多代谢反应,已在OA、肝病和抑郁症的背景下进行了研究。一些证据表明,它可以通过减少炎症介质和促进软骨合成来缓解疼痛并改善关节功能51。在一项涉及约100名髋关节、膝关节和脊椎OA患者的长期多中心试验中,接受600mg SAMe治疗两周,然后每天400mg,持续24个月,SAMe改善了临床症状,如晨僵和疼痛,以及抑郁症状52。
在一项随机、双盲、交叉研究中,61名膝关节骨性关节炎患者每天接受1200mg SAMe或200mg塞来昔布治疗,为期16周。在第一个月结束时,塞来昔布显示疼痛评分明显降低。到第二个月底,两个治疗组之间没有差异。两组患者的关节健康状况也有所改善。研究人员得出结论,SAMe在治疗膝盖OA症状方面与塞来昔布一样有效53。
9. 维生素D:
维生素D是一种脂溶性维生素,在骨骼健康、细胞生长、免疫功能和对抗炎症方面发挥作用。维生素D的来源包括阳光照射和高脂肪鱼类、牛肉肝、奶酪和蛋黄等食物54。
在一项随机对照试验中,103名缺乏维生素D的膝关节骨性关节炎患者接受了60,000IU的维生素D或安慰剂治疗,每天一次、持续10天,然后,60,000IU每月一次,为期12个月。治疗组的患者报告疼痛减轻,功能改善55。一项病例对照研究检查了饮食营养素与膝关节骨性关节炎之间的关系,发现维生素C和D的摄入量较低与骨性关节炎显著相关。虽然需要更多的研究来阐明饮食在OA发作和进展中的作用,但维生素C和D的低摄入量可能是一个风险因素56。
最近一项针对1136名膝关节骨性关节炎患者的四项随机临床试验的荟萃分析发现,补充超过2000IU的维生素D可以减轻疼痛,增强功能,但不能防止软骨损伤57。在另一项研究中,340名膝关节骨关节炎患者在基线、3个月、6个月、12个月和24个月时测量了维生素D状态。与维生素D水平不足的组相比,维生素D持续充足的组胫骨软骨损失较少,身体功能改善58。
10. 维生素E:
维生素E是一种脂溶性维生素和强效抗氧化剂,对免疫健康也起着至关重要的作用。维生素E天然存在于坚果、种子和绿叶蔬菜中59。维生素E具有抗炎作用,有助于预防OA。最近一篇关于临床前和临床研究的文献综述表明,维生素E可以减少软骨细胞的氧化应激,而动物研究表明维生素E可以防止软骨降解。一些对人类的观察性研究将低维生素E水平与OA联系起来60。另一项临床前研究综述表明,维生素E可能通过维持骨骼肌和调节OA发病基因的表达来减缓OA的进展61。
在一项随机双盲研究中,15只患有OA的狗每天接受400IU维生素E或安慰剂治疗55天。治疗组的跛行、疼痛、软骨损伤和滑液中的炎症标志物均有改善62。
一项涉及23名膝关节OA患者的研究发现,滑液中维生素E的浓度与OA的严重程度呈负相关63。在另一项研究中,40名健康受试者和40名膝关节骨性关节炎患者接受了200mg维生素E或安慰剂治疗,为期三个月。服用维生素E的组的炎症标志物水平较低,这可能会防止氧化应激引起的关节恶化64。
11. 菠萝蛋白酶:
已知菠萝蛋白酶具有抗炎特性,被用于对抗鼻腔肿胀、炎症和肌肉酸痛65。最近的证据表明,它可能有助于缓解OA的症状。在一项随机、单盲、对照试验中,40名膝关节骨性关节炎患者服用500mg菠萝蛋白酶或100mg双氯芬酸,为期四周。研究人员发现,与基线值相比,两个治疗臂的疼痛、僵硬和功能都有所改善66。
在一项观察性、前瞻性、开放标签研究中,一组慢性OA疼痛患者和另一组急性OA疼痛患者(共42名受试者)服用了魔爪草、姜黄和菠萝蛋白酶的组合。治疗包括慢性疼痛患者服用两粒650mg胶囊,每日三次,持续60天,急性疼痛患者服用650mg胶囊每日两次,持续15天。两组患者的关节疼痛均有改善67。
12. 硼:
已知硼有助于骨骼和肌肉健康,并减少与OA相关的炎症、关节僵硬和其他症状68。一项涉及43名膝关节OA患者的对照研究确定,与健康对照组相比,OA患者的硼水平明显较低。血清硼水平较低也与OA持续时间和严重程度增加有关69。尚需要更多的研究来更好地了解硼在对抗炎症和OA中的作用。
13.姜黄素:
姜黄素具有强大的抗炎特性70,补充可能有助于缓解与OA相关的疼痛和症状71。
一项涉及40名轻度至中度膝关节骨性关节炎患者的随机、双盲、安慰剂对照试验表明,与安慰剂相比,每天1500mg的姜黄素减轻了疼痛,改善了身体功能评分72。在另一项随机、安慰剂对照、双盲研究中,50名40岁以上膝关节骨性骨折患者接受了每天180mg的姜黄素或安慰剂治疗。八周后,治疗组报告的膝盖疼痛明显少于安慰剂组73。动物模型研究也支持姜黄素的抗炎和软骨保护作用。在一项研究中,作者得出结论,提取物甚至可能改变OA的进展74。
14. 乳香:
乳香是一种生长在印度、北非和中东山区的树,传统上用于宗教和文化目的。这种树的树脂提取物已被证明具有强大的抗炎特性75。乳香可能在缓解哮喘、关节炎和克罗恩病方面发挥作用。其生物活性被认为至少部分归因于乳香酸(Boswellic acids)70。
较早的随机临床研究表明,这种提取物在治疗OA中的作用(每天三次,每次333mg提取物或100或250mg 30%乳香酸的提取物)76,77。最近,在一项随机、双盲、安慰剂对照的研究中,60名OA患者服用了乳香(100mg)或安慰剂,持续30天。治疗组在疼痛和身体机能方面有了显著的改善,这在试验开始的第5天就得到了证明78。动物研究也表明口服和外用乳香治疗对OA患者都有治疗作用79。
研究表明,乳香可能与其他草药提取物结合使用是有用的。在最近的一项随机双盲研究中,201名OA患者接受安慰剂,333mg姜黄素,或500mg含有250mg姜黄素和150mg乳香酸的胶囊,每天三次,持续12周。对患者的身体功能和疼痛进行了评估,结果表明,采用联合治疗的患者疼痛缓解程度最高80。另一项对28名中度OA患者的随机研究比较了姜黄和乳香联合用药500mg、每日两次和100mg塞来昔布、每日两次,持续12周。与塞来昔布组相比,乳香-姜黄组在报告的疼痛、步行距离和关节线压痛方面有更大的改善。这种治疗也被发现是安全且耐受性良好的70。
15. 姜根(生姜):
生姜传统上用作香料和治疗胃肠道问题。一些证据表明,它的抗炎特性可能有助于对抗OA81。一项较早的随机、双盲、安慰剂对照试验评估了261名经历中度至重度疼痛的膝关节OA患者。受试者每天两次接受生姜提取物或安慰剂治疗,并允许将对乙酰氨基酚作为应急药物。与安慰剂组相比,治疗组在站立或行走50英尺后膝盖疼痛减轻得更多,对乙酰氨基酚的需求频率更低82。
在一项随机、双盲、安慰剂对照试验中,120名OA患者被分为三组:一组接受30mg生姜提取物(两粒500mg胶囊),另一组接受安慰剂,第三组每天服用三片400mg布洛芬。生姜提取物和布洛芬在改善症状(包括疼痛和关节运动)方面同样有效83。在另一项随机临床试验中,204名膝关节骨性关节炎患者在六周内每天两次服用250mg生姜粉或安慰剂。与安慰剂组相比,治疗组的患者在疼痛和僵硬方面表现出更显著的改善84。
16. 碧萝芷:
来源于法国海岸的海松树皮专利提取物—碧萝芷,具有强大的抗炎和抗氧化特性85。临床前研究表明碧萝芷可能抑制蛋白酶(降解软骨的酶),三项临床研究表明它可以减轻疼痛和僵硬86。
一项随机试点研究涉及33名严重OA患者,他们在膝关节置换术前三周接受每天两次的100mg碧萝芷治疗或不接受治疗。研究人员随后检查了血清和滑液中的软骨稳态标志物和炎症介质。碧萝芷下调了与软骨降解相关的基因并降低炎症标记物87。
17. 肉豆蔻酸酯(CMO):
CMO又称十六烷基化脂肪酸(Cetylated Fatty Acids)或鲸蜡醇酯,具有抗炎、保护关节作用。产品形式通常有口服和外用二种。在一项随机、双盲、安慰剂对照研究中,Celadrin(CMO原料品牌)对膝关节骨性关节炎 的影响。40名患者每天二次使用安慰剂或Celadrin乳霜,持续30天。Celadrin受试者在坐下、坐下后站起来、爬楼梯和平衡的能力以及膝关节活动能力都有所改善。研究者结论:“使用CMO外用乳膏是改善膝关节ROM、上/下楼梯的能力、坐起、行走和坐下的能力以及单侧平衡能力的有效治疗方法。”88
一项随机、双盲、安慰剂对照研究测试了Celadrin对膝关节OA的益处。共有64名参与者每天服用6粒安慰剂或Celadrin(350mg)胶囊,持续68天,并评估了他们的膝关节功能。Celadrin组在膝关节屈曲和Lequesne算法功能指数(LAI)方面有所改善,这是一种衡量膝关节功能和疼痛的指标。研究人员得出结论,“CMO可以替代使用非甾体抗炎药治疗OA。”89
18. 橄榄油(局部使用)
橄榄油富含植物营养素,局部使用有助于减轻疼痛和炎症。2012年,一项为期四周的临床试验在30名40-85岁患有膝关节炎的女性中比较了局部使用的橄榄油和吡罗西康(一种局部使用的非甾体抗炎药)。据报道,那些接受橄榄油的人在疼痛和身体机能方面比介绍吡罗西康的人有更大的改善90。在一项涉及16名女性和14名男性膝关节OA患者的随机研究中,受试者被分配到两组,一组接受局部特级初榨橄榄油和锻炼计划,一组接受局部非甾体抗炎药(酮洛芬凝胶)和锻炼计划,另一组每天只进行三次锻炼。治疗每周进行五天,为期两周。所有组均表现出OA症状的显著改善,橄榄油组和局部非甾体抗炎药组在缓解疼痛方面的效果优于单独运动91。
更多内容可点击其个性化的综合干预方案如下:
- 关节炎管理(保护关节)
- 关节炎管理(维持关节灵活)
- 关节炎管理(抗炎止痛)
- 关节炎管理(局部止痛)
- 关节炎管理(防药物副作用)
- 骨关节退化防控(50-60岁)
- 骨关节退化防控(61-70岁)
- 骨关节退化防控(71-80岁)
- 骨关节退化防控(81岁以上)
骨质增生或骨关节炎防控:
以及参阅本网如下专文的有关内容:
医疗干预
治疗的目的是减少关节疼痛和炎症,改善关节功能。
常规治疗包括如下:
- 管理疼痛或减轻炎症的药物,包括如下:
- 非甾体类抗炎药(NSAIDs),如对乙酰氨基酚、布洛芬和萘普生等。
- 外用止痛药,如卡宴椒药膏
- 阿片类药物和类似药物
- 糖皮质激素,可以通过口服或注射
- 注射透明质酸,增加关节灵活
- 其他可能治疗包括:
- 经皮神经电刺激(TENS),电脉冲可以减少疼痛信号
- 人工治疗,如按摩改善肌肉和关节的平衡。
其他疗法
- 减肥:可以减轻超重或肥胖者关节应力,缓解OA症状。
- 运动与理疗:
- 强化肌肉与力量:肌肉可影响关节的排列、抵抗外力等。肌肉越强,运动时关节磨损就越少。
- 加强支持关节的肌肉:可以减少疼痛和改善运动。
- 合适的运动锻炼形式,运动对关节的损伤和保护作用也不同。例如,游泳和水中有氧运动可改善肌肉健康,对关节的影响较小。
- 物理或职业治疗:可提供一些设备来帮助完成日常任务,例如:
- 带减震底的鞋子。
- 夹板或支架有助于正确对齐关节点和合理分配重量。
- 弹性支承。
- 手杖、拐杖、助行器和矫形鞋。
- 改善家里使用的器具,如升高座椅、马桶,增加一些扶手等。
- 热、冰疗法:
- 热疗可以帮助放松僵硬的关节和改善运动,如使用热水袋、温水浸泡、石蜡或加热垫。
- 敷冰可能有助于减轻运动后的关节肿胀和疼痛。
预防
有助于降低骨关节炎的措施包括:- 保持健康的体重。
- 定期运动,如散步、游泳、瑜伽或伸展、拉伸等。
- 避免重复的动作,以免导致关节损伤,尤其在40岁以后。
参考文献:
1. Sanders M et al. The use of glucosamine, devil's claw (Harpagophytum procumbens), and acupuncture as complementary and alternative treatments for osteoarthritis. Alternative medicine review : a journal of clinical therapeutic. 2011;16(3):228-238.
2. Aghazadeh-Habashi A et al. The glucosamine controversy; a pharmacokinetic issue. Journal of pharmacy & pharmaceutical sciences. 2011;14(2):264-273.
3. Reginster JY et al. Role of glucosamine in the treatment for osteoarthritis. Rheumatology international. 2012;32(10):2959-2967.
4. Fouladbakhsh J. Complementary and alternative modalities to relieve osteoarthritis symptoms. Am J Nurs. 2012;112(3 Suppl 1):S44-51.
5. Martel-Pelletier J et al. Discrepancies in composition and biological effects of different formulations of chondroitin sulfate. Molecules (Basel, Switzerland). 2015;20(3):4277-4289.
6. Ishimaru D et al. Alterations in the chondroitin sulfate chain in human osteoarthritic cartilage of the knee. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society. 2014;22(2):250-258.
7. Calamia V et al. A pharmacoproteomic study confirms the synergistic effect of chondroitin sulfate and glucosamine. Sci Rep. 2014;4:5069.
8. Zegels B et al. Equivalence of a single dose (1200 mg) compared to a three-time a day dose (400 mg) of chondroitin 4&6 sulfate in patients with knee osteoarthritis. Results of a randomized double blind placebo controlled study. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society. 2013;21(1):22-27.
9. Gabay C et al. Symptomatic effects of chondroitin 4 and chondroitin 6 sulfate on hand osteoarthritis: a randomized, double-blind, placebo-controlled clinical trial at a single center. Arthritis and rheumatism. 2011;63(11):3383-3391.
10. Hochberg MC et al. Combined chondroitin sulfate and glucosamine for painful knee osteoarthritis: a multicentre, randomised, double-blind, non-inferiority trial versus celecoxib. Ann Rheum Dis. 2016;75(1):37-44.
11. Martel-Pelletier J et al. Levels of serum biomarkers from a two-year multicentre trial are associated with treatment response on knee osteoarthritis cartilage loss as assessed by magnetic resonance imaging: an exploratory study. Arthritis Res Ther. 2017;19(1):169.
12. Pelletier JP et al. Chondroitin sulfate efficacy versus celecoxib on knee osteoarthritis structural changes using magnetic resonance imaging: a 2-year multicentre exploratory study. Arthritis Res Ther. 2016;18(1):256.
13. Fransen M et al. Glucosamine and chondroitin for knee osteoarthritis: a double-blind randomised placebo-controlled clinical trial evaluating single and combination regimens. Ann Rheum Dis. 2015;74(5):851-858.
14. Papakonstantinou E et al. Hyaluronic acid: A key molecule in skin aging. Dermatoendocrinol. 2012;4(3):253-258.
15. Ricci M et al. Clinical comparison of oral administration and viscosupplementation of hyaluronic acid (HA) in early knee osteoarthritis. Musculoskelet Surg. 2017;101(1):45-49.
16. Martinez-Puig D et al. Efficacy of oral administration of yoghurt supplemented with a preparation containing hyaluronic acid (Mobilee™) in adults with mild joint discomfort: a randomized, double-blind, placebo-controlled intervention study. Mediterranean Journal of Nutrition and Metabolism. 2013;6(1):63-68.
17. Kalman DS et al. Effect of a natural extract of chicken combs with a high content of hyaluronic acid (Hyal-Joint®) on pain relief and quality of life in subjects with knee osteoarthritis: a pilot randomized double-blind placebo-controlled trial. Nutrition journal. 2008;7(1):3.
18. Arthritis Foundation. Avocado Soybean Unsaponifiables (ASU). https://www.arthritis.org/living-with-arthritis/treatments/natural/supplements-herbs/guide/avocado-soybean.php. Accessed July 10, 2019.
19. Christiansen BA et al. Management of Osteoarthritis with Avocado/Soybean Unsaponifiables. Cartilage. 2015;6(1):30-44.
20. Catunda IS et al. Clinical effects of an avocado-soybean unsaponifiable extract on arthralgia and osteoarthritis of the temporomandibular joint: preliminary study. International journal of oral and maxillofacial surgery. 2016;45(8):1015-1022.
21. Maheu E et al. Randomised, controlled trial of avocado-soybean unsaponifiable (Piascledine) effect on structure modification in hip osteoarthritis: the ERADIAS study. Ann Rheum Dis. 2014;73(2):376-384.
22. Loef M et al. Fatty acids and osteoarthritis: different types, different effects. Joint, bone, spine : revue du rhumatisme. 2019;86(4):451-458.
23. Bahamondes MA et al. Effect of omega-3 on painful symptoms of patients with osteoarthritis of the synovial joints: systematic review and meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol. Sep 2021;132(3):297-306.
24. Wu CL et al. Dietary fatty acid content regulates wound repair and the pathogenesis of osteoarthritis following joint injury. Ann Rheum Dis. 2015;74(11):2076-2083.
25. Moreau M et al. Effects of feeding a high omega-3 fatty acids diet in dogs with naturally occurring osteoarthritis. Journal of animal physiology and animal nutrition. 2013;97(5):830-837.
26. Elagizi A et al. An Update on Omega-3 Polyunsaturated Fatty Acids and Cardiovascular Health. Nutrients. Jan 12 2021;13(1)
27. Harris WS et al. The Omega-3 Index and relative risk for coronary heart disease mortality: Estimation from 10 cohort studies. Atherosclerosis. Jul 2017;262:51-54.
28. McBurney MI et al. Using an erythrocyte fatty acid fingerprint to predict risk of all-cause mortality: the Framingham Offspring Cohort. Am J Clin Nutr. Oct 4 2021;114(4):1447-1454.
29. Ma MY et al. Omega-3 index and type 2 diabetes: Systematic review and meta-analysis. Prostaglandins Leukot Essent Fatty Acids. Nov 2021;174:102361.
30. Demonty I et al. Proportions of long-chain ω-3 fatty acids in erythrocyte membranes of Canadian adults: Results from the Canadian Health Measures Survey 2012-2015. Am J Clin Nutr. Apr 6 2021;113(4):993-1008.
31. Schuchardt JP et al. Red blood cell fatty acid patterns from 7 countries: Focus on the Omega-3 index. Prostaglandins, Leukotrienes and Essential Fatty Acids. 2022 Apr;179:102418.
32. Stonehouse W et al. Krill oil improved osteoarthritic knee pain in adults with mild to moderate knee osteoarthritis: a 6-month multicenter, randomized, double-blind, placebo-controlled trial. Am J Clin Nutr. 2022 Sep 2;116(3):672-685.
33. Ulven SM et al. Comparison of bioavailability of krill oil versus fish oil and health effect. Vasc Health Risk Manag. 2015;11:511-24.
34. Huang LJ et al. Astaxanthin ameliorates cartilage damage in experimental osteoarthritis. Modern rheumatology / the Japan Rheumatism Association. Sep 2015;25(5):768-71.
35. Strasser H. [On standarization in the breeding and keeping of experimental animals]. Berl Munch Tierarztl Wochenschr. Mar 1 1966;79(5):91-6. Zur Standardisierung in der Versuchstierzucht und -haltung.
36. Suzuki Y et al. Krill Oil Improves Mild Knee Joint Pain: A Randomized Control Trial. PLoS One. 2016;11(10):e0162769.
37. Laslett LL et al. Efficacy of krill oil in the treatment of knee osteoarthritis: a 24-week multicentre randomised double-blind controlled trial. Osteoarthritis and Cartilage. 2021;29:S10-S11.
38. Di Lullo GA et al. Mapping the ligand-binding sites and disease-associated mutations on the most abundant protein in the human, type I collagen. J Biol Chem. 2002;277(6):4223-4231.
39. Kumar S et al. A double-blind, placebo-controlled, randomised, clinical study on the effectiveness of collagen peptide on osteoarthritis. Journal of the science of food and agriculture. 2015;95(4):702-707.
40. Zhao W et al. Chicken type II collagen induced immune tolerance of mesenteric lymph node lymphocytes by enhancing beta2-adrenergic receptor desensitization in rats with collagen-induced arthritis. International immunopharmacology. 2011;11(1):12-18.
41. Cohen ES et al. Cytotoxic T lymphocytes recognize and lyse chondrocytes under inflammatory, but not non-inflammatory conditions. Immunology. 2003;109(1):8-14.
42. Bagchi D et al. Effects of orally administered undenatured type II collagen against arthritic inflammatory diseases: a mechanistic exploration. International journal of clinical pharmacology research. 2002;22(3-4):101-110.
43. Crowley DC, Lau FC, Sharma P, et al. Safety and efficacy of undenatured type II collagen in the treatment of osteoarthritis of the knee: a clinical trial. Int J Med Sci. 2009;6(6):312-321.
44. Bakilan F et al. Effects of Native Type II Collagen Treatment on Knee Osteoarthritis: A Randomized Controlled Trial. Eurasian J Med. 2016;48(2):95-101.
45. Lugo JP et al. Efficacy and tolerability of an undenatured type II collagen supplement in modulating knee osteoarthritis symptoms: a multicenter randomized, double-blind, placebo-controlled study. Nutr J. 2016;15(1):14.
46. Ezaki J et al. Assessment of safety and efficacy of methylsulfonylmethane on bone and knee joints in osteoarthritis animal model. Journal of bone and mineral metabolism. 2013;31(1):16-25.
47. Debbi EM et al. Efficacy of methylsulfonylmethane supplementation on osteoarthritis of the knee: a randomized controlled study. BMC Complement Altern Med. 2011;11:50.
48. Kim LS et al. Efficacy of methylsulfonylmethane (MSM) in osteoarthritis pain of the knee: a pilot clinical trial. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society. 2006;14(3):286-294.
49. A Pagonis T et al. The Effect of Methylsulfonylmethane on Osteoarthritic Large Joints and Mobility. International Journal of Orthopaedics. 2014;1:1-6.
50. Vidyasagar S et al. Efficacy and Tolerability of Glucosamine - Chondroitin Sulphate - Methyl Sulfonyl Methane (MSM) in Osteoarthritis of Knee in Indian Patients. iums-ijpt. 2004;3(2):61-60.
51. Hosea Blewett HJ. Exploring the mechanisms behind S-adenosylmethionine (SAMe) in the treatment of osteoarthritis. Crit Rev Food Sci Nutr. 2008;48(5):458-463.
52. Konig B. A long-term (two years) clinical trial with S-adenosylmethionine for the treatment of osteoarthritis. Am J Med. 1987;83(5A):89-94.
53. Najm WI et al. S-adenosyl methionine (SAMe) versus celecoxib for the treatment of osteoarthritis symptoms: a double-blind cross-over trial. [ISRCTN36233495]. BMC Musculoskelet Disord. 2004;5(1):6.
54. U.S. NIH ods. Vitamin D. https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/. Published 2018. Accessed July 6, 2019.
55. Sanghi D et al. Does vitamin D improve osteoarthritis of the knee: a randomized controlled pilot trial. Clin Orthop Relat Res. 2013;471(11):3556-3562.
56. Sanghi D et al. Elucidation of dietary risk factors in osteoarthritis knee-a case-control study. J Am Coll Nutr. 2015;34(1):15-20.
57. Gao XR et al. The effect of vitamin D supplementation on knee osteoarthritis: A meta-analysis of randomized controlled trials. International journal of surgery (London, England). 2017;46:14-20.
58. Zheng S et al. Maintaining Vitamin D Sufficiency Is Associated with Improved Structural and Symptomatic Outcomes in Knee Osteoarthritis. Am J Med. 2017;130(10):1211-1218.
59. U.S. National Library of Medicine. Vitamin E. https://medlineplus.gov/ency/article/002406.htm. Published 2019.
60. Chin KY et al. The Role of Vitamin E in Preventing and Treating Osteoarthritis - A Review of the Current Evidence. Frontiers in pharmacology. 2018;9:946.
61. Li XI et al. Vitamin E slows down the progression of osteoarthritis. Experimental and therapeutic medicine. 2016;12(1):18-22.
62. Rhouma M et al. Anti-inflammatory response of dietary vitamin E and its effects on pain and joint structures during early stages of surgically induced osteoarthritis in dogs. Can J Vet Res. 2013;77(3):191-198.
63. Angthong C et al. Can levels of antioxidants in synovial fluid predict the severity of primary knee osteoarthritis: a preliminary study. Springerplus. 2013;2:652.
64. Bhattacharya I et al. Efficacy of vitamin E in knee osteoarthritis management of North Indian geriatric population. Therapeutic advances in musculoskeletal disease. 2012;4(1):11-19.
65. U.S. NIH: NCCIH. Bromelain. https://nccih.nih.gov/health/bromelain. Published 2016.
66. Kasemsuk T et al. Improved WOMAC score following 16-week treatment with bromelain for knee osteoarthritis. Clin Rheumatol. 2016;35(10):2531-2540.
67. Conrozier T et al. A complex of three natural anti-inflammatory agents provides relief of osteoarthritis pain. Alternative therapies in health and medicine. 2014;20 Suppl 1:32-37.
68. Mahmood N. Relationship between Serum Levels of Some Trace Elements, Disease Duration and Severity in Patients with Knee Osteoarthritis. Vol 062015.
69. Naza Mohammad Ali Mahmood1 ORB, Saad Abdulrahman Hussain3 IRAQ. Relationship between serum concentrations of boron and inflammatory markers, disease duration, and severity of patients with knee osteoarthritis in Sulaimani city. National Journal of Physiology, Pharmacy and Pharmacology. 2015;6(1).
70. Kizhakkedath R. Clinical evaluation of a formulation containing Curcuma longa and Boswellia serrata extracts in the management of knee osteoarthritis. Molecular medicine reports. 2013;8(5):1542-1548.
71. Chin KY. The spice for joint inflammation: anti-inflammatory role of curcumin in treating osteoarthritis. Drug design, development and therapy. 2016;10:3029-3042.
72. Panahi Y et al. Curcuminoid treatment for knee osteoarthritis: a randomized double-blind placebo-controlled trial. Phytother Res. 2014;28(11):1625-1631.
73. Nakagawa Y et al. Short-term effects of highly-bioavailable curcumin for treating knee osteoarthritis: a randomized, double-blind, placebo-controlled prospective study. J Orthop Sci. 2014;19(6):933-939.
74. Zhang Z et al. Curcumin slows osteoarthritis progression and relieves osteoarthritis-associated pain symptoms in a post-traumatic osteoarthritis mouse model. Arthritis research & therapy. 2016;18(1):128.
75. Siddiqui MZ. Boswellia serrata, a potential antiinflammatory agent: an overview. Indian journal of pharmaceutical sciences. 2011;73(3):255-261.
76. Thawani V et al. Open, randomized, controlled clinical trial of <i> Boswellia serrata </i> extract as compared to valdecoxib in osteoarthritis of knee. Indian journal of pharmacology. 2007;39(1):27-29.
77. Sengupta K et al. A double blind, randomized, placebo controlled study of the efficacy and safety of 5-Loxin for treatment of osteoarthritis of the knee. Arthritis research & therapy. 2008;10(4):R85.
78. Vishal AA et al. A double blind, randomized, placebo controlled clinical study evaluates the early efficacy of aflapin in subjects with osteoarthritis of knee. Int J Med Sci. 2011;8(7):615-622.
79. Wang Q et al. Oral and topical boswellic acid attenuates mouse osteoarthritis. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society. 2014;22(1):128-132.
80. Haroyan A et al. Efficacy and safety of curcumin and its combination with boswellic acid in osteoarthritis: a comparative, randomized, double-blind, placebo-controlled study. BMC Complement Altern Med. 2018;18(1):7.
81. Mashhadi NS et al. Anti-oxidative and anti-inflammatory effects of ginger in health and physical activity: review of current evidence. International journal of preventive medicine. 2013;4(Suppl 1):S36-42.
82. Altman RD et al. Effects of a ginger extract on knee pain in patients with osteoarthritis. Arthritis and rheumatism. 2001;44(11):2531-2538.
83. Haghighi M et al. Comparing the Effects of ginger (Zingiber officinale) extract and ibuprofen On patients with osteoarthritis. Vol 82005.
84. Zakeri Z et al. Evaluating the effects of ginger extract on knee pain, stiffness and difficulty in patients with knee osteoarthritis. Vol 52011.
85. Center MSKC. Pine Bark Extract. https://www.mskcc.org/cancer-care/integrative-medicine/herbs/pine-bark-extract. Published 2018.
86. Rohdewald PJ. Review on Sustained Relief of Osteoarthritis Symptoms with a Proprietary Extract from Pine Bark, Pycnogenol. Journal of medicinal food. 2018;21(1):1-4.
87. Jessberger S et al. Cellular pharmacodynamic effects of Pycnogenol(R) in patients with severe osteoarthritis: a randomized controlled pilot study. BMC Complement Altern Med. 2017;17(1):537.
88. Kraemer WJ et al. Effect of a cetylated fatty acid topical cream on functional mobility and quality of life of patients with osteoarthritis. J Rheumatol. 2004 Apr;31(4):767-74.
89. Hesslink R Jr et al. Cetylated fatty acids improve knee function in patients with osteoarthritis. J Rheumatol. 2002 Aug;29(8):1708-12.
90. Bohlooli S et al. A pilot double-blinded, randomized, clinical trial of topical virgin olive oil versus piroxicam gel in osteoarthritis of the knee. J Clin Rheumatol. 2012;18(2):99-101.
91. AL MALTY A-Mea. The effect of Topical Application of Extra Virgin Olive Oil on Alleviating Knee Pain in Patients with Knee Osteoarthritis: A Pilot Study. Indian Journal of Physiotherapy & Occupational Therapy-An International Journal. 2013:6-11.
参考来源:
美国梅奥诊所
www.mayoclinic.org
美国关节炎基金会
http://www.arthritis.org
美国国立公众健康网
www.medlineplus.gov
美国风湿病学会
http://www.rheumatology.org
加拿大关节炎协会
http://www.arthritis.ca
加拿大老年健康网
http://www.seniors.gc.ca
其他参考文献:详见具体的综合干预方案
免责声明和安全信息
- 本信息(包括任何附带资料)不是为了取代医生或有关合格从业人士的建议或忠告。
- 任何人如果想要对本文涉及的药物、饮食、运动或其他生活方式的使用、或改变调整,以预防或治疗某一特定健康状况或疾病,应首先咨询医生或有关合格从业人士,并获得他/她们的许可。妊娠和哺乳妇女在使用本网站任何内容前,尤其应征求医生的意见。
- 除非另有说明,本网站所述内容仅适用于成人。
- 本网站所推荐的任何产品,消费者应该以实际的产品标签内容为准,尤其应关注重要的安全信息以及产品最新信息,包括剂量、使用方法和禁忌症等。
- 由于循证医学研究、文献及有关产品处于不断的变化中,本网站工作人员将尽力更新。
- 本网站不能保证所载文章内容、综合干预方案以及相关成分或产品述及的健康益处,也不承担任何责任。